
In calculating your ideal body weight, physicians use a formula called the Body Mass Index (BMI),
which is a number that expresses the relationship between your height and weight.
resources
Links and References

Finance and Insurance
Nutrient Fortified Protein Foods and Meals
www.obesitycenter.tsfl.com
American Society for Bariatric Surgery
www.asbs.org
National Institutes of Health on Surgery for Obesity
www.niddk.nih.gov/health/nutrit/pubs/
Walter Lindstrom's Obesity Law Center
www.obesitylaw.com
Olwen's Links
http://crash.ihug.co.nz/~olwen/ocwlnkws.htm
Obesity Help
www.obesityhelp.com
George Washington University
www.gwhospital.com
MAC Pharma Network
www.mac-pharma-network.net
Refererences
Drenick EJ, Blae GF, Seltzer F. Excessive mortality and causes of death in morbidly obese men. JAMA 1980; 243; 443-445
Benotti PN, Hollingshead J., Mascioli EA. Gastric Restrictive Operations for Morbid Obesity AM J. Surg. 1989; 157: 150-155
Pories WJ, MacDonald KG Jr., Morgan EJ, et al. Surgical Treatment of Obesity and its effects on Diabetes: 10 year follow-up. AM J Nutr 1992; 55:615S-9S
Mason EE. Gastric Bypass. Ann Surg; 1969: 229-233
Gastrointestinal Surgery for Severe Obesity: National Institutes of Health Consensus Development Conference Statement.
Shamblin Jr. Shamblin WR Bariatric Surgery Should Be More Widely Accepted. South Med J 1987; 80:861-865
Sugarman JH, Starkey JV. A random prospective trial of gastric bypass versus vertical banded gastroplasty versus non-sweet eaters. Ann Surg 1987; 207: 613-624
Rand CS, MacGregor AMC, Hankins GC. Gastric Bypass Surgery for Obesity: Weight loss, Psychosocial outcome and morbidity one and three years later. South Med J 1986; 79: 1511-1514
Information on Body Mass Index (BMI)
In calculating your ideal body weight, physicians use a formula called the Body Mass Index (BMI), which is a number that expresses the relationship between your height and weight.
The BMI calculator below will determine your individual BMI
Body Mass Index is interpreted as follows:
| <20 | Underweight |
| 20 - 24.9 | 20-24.9 Ideal Weight |
| 25 - 29.9 | Overweight |
| 30 - 39.9 | Obese |
| 40> | Morbidly Obese |
surgery options
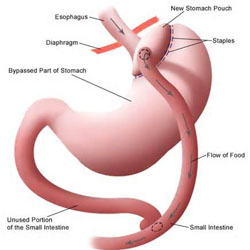
LAPAROSCOPIC ROUX-EN-Y GASTRIC BYPASS
In this operation the stomach is divided into two compartments with several rows of titanium staples.Read More
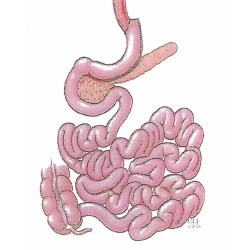
LAPAROSCOPIC SLEEVE GASTERECTOMY
The Laparoscopic Sleeve Gastrectomy - often called the sleeve - is performed by removing approximately 80 percent of the stomach. Read More

REVISION BARIATRIC SURGERY
Failure of Bariatric procedures can happen 3-7% of all Bariatric Surgery. Read More
As with any major abdominal surgery there are potential risks. These risks can be further complicated in operations on severely obese patients. It is important that you consider these potential risks, and discuss them with Dr. Afram and your own physician, when deciding whether to have surgery. Potential surgical risks include possible respiratory problems, infections, bleeding, bowel obstruction, leakage of the bowel connections, and obstruction of the stomach outlet. After performing over 3000 gastric bypass operations, Dr. Afram and his team have developed successful strategies for minimizing any potential risks.
POTENTIAL SIDE EFFECTS OF THE SURGERY
Due to the physical changes caused by the gastric bypass surgery, there are potential side effects that result from the surgery and your new way of eating. Due to restricted eating, there is a potential for deficiencies in protein, as well as certain vitamins and minerals. Use of an over-the-counter multivitamin, fortified with iron and calcium, and other nutritional supplements, determined on an individual basis, can help mitigate this risk.
Some patients experience nausea, food intolerance, changed bowel habits, transient hair loss, and loss of muscle mass. It is important to note that not all patients experience these side effects and these side effects are usually transitory. If you experience any of these post-operative side effects, Dr. Afram and the nutritionist are available for immediate consultation.
Gall bladder disease is a potential side effect due to the rapid weight loss most patients experience after the surgery. To minimize this risk Dr. Afram may prescribe medication, taken regularly for several months after surgery.
A word about pregnancy.
Infertility can be a significant co-morbidity for severely obese women. Many obese women experience irregular or non-existent menstrual cycles. Surgery for obesity often corrects these problems. Due to the increased nutritional needs of pregnancy, we recommend that patients not get pregnant for at least one to two years after surgery, when the initial rapid weight loss subsides. Patients should discuss birth control methods with their primary care physician or obstetrician/gynecologist. After the initial year, pregnancy is safe and many patients, who had suffered from infertility prior to surgery, have delivered healthy babies.
RESULTS
Most of our patients are very satisfied with the results of their operation. Overwhelmingly, patients have found that they lose 50 to 90 percent of their excess weight, and maintain that weight loss long-term.
Maximum effectiveness depends on the level of patient participation in the behavioral modification and nutritional programs, as well as an increase in physical activities and exercise on a regular basis. Other factors, such as age, sex, and initial weight at the time of surgery should also be considered. Weight loss surgery is not a magic bullet. It is, however, a powerful tool that has successfully helped many people achieve and maintain permanent weight loss. Your active participation in, and commitment to, the life style changes, exercise, and eating habits that weight loss surgery requires is a necessary component to your ultimate success.
Most medical diseases are improved or cured. Obesity related diseases are improved dramatically.
- High Blood Pressure can be often alleviated or eliminated by weight loss surgery
- High Blood Cholesterol in 80% of the patients can be alleviated or eliminated and in as little as 2-3 months post-operatively
- Heart Disease in obese individuals is certainly more likely to be experienced when compared to persons who are of average weight and adhere to a strict diet and exercise regimen. There is no hard and fast statistical data to definitively prove that weight loss surgery reduces the risk of cardiovascular disease, however, common sense would dictate that if we can significantly reduce many of the co-morbidities that we experienced as someone that is obese, we can likewise that our health may be much improved if not totally restored.
- Diabetes Mellitus can be cured or tremendously improved. Complications can be controlled based on many post gastric bypass studies.
- Abnormal Glucose Tolerance, or "Borderline Diabetes" is even more likely reversed by Gastric Bypass. Since this condition becomes diabetes in many cases, the operation can frequently prevent diabetes as well
- Asthma sufferers may find that they have fewer and less severe attacks, or sometimes none at all. When asthma is associated with gastroesophageal reflux disease, it is particularly benefited by gastric bypass.
- Sleep Apnea Syndrome sufferers can receive dramatic effects and many within a year or so of surgery find their symptoms were completely gone and they ever stopped snoring completely!
- Gastroesophageal Reflux Disease can be greatly relieved of all symptoms within as little as a few days of surgery
- Gallbladder Disease can be surgically handled at the time of weight loss surgery if your doctor has cause to believe that gallstones are present.
- Stress Urinary Incontinence responds dramatically to weight loss, usually by becoming completely controlled. A person who is still troubled by incontinence can choose to have specific corrective surgery later, with much greater chance of a successful outcome, with a reduced body weight.
- Low Back Pain and Degererative Disk Disease, and Degenerative Joint Disease can be considerable relieved with weight loss, and greater comfort may be experienced even after as few as 30 pounds are lost.
- Major improvement in the quality of life and improvement in self-esteem and self-confidence.










